Diabetes Type 1
Current Approaches in Patient Management for Individuals Diagnosed with Type 1 Diabetes
Online Continuing Education Course

Course Description
2.5-contact-hour diabetes CEU course on type 1 diabetes mellitus (T1DM). Identify development, diagnosis, treatment regimens, management, and interventions to avoid acute and chronic complications. Applicable for nursing, occupational therapy, and other healthcare professionals.
Course Price: $11.00
Original Price: $22.00
Exclusive 50% Discount
Contact Hours: 2.5
Pharmacotherapeutic Hours: 0.25
Course updated on
October 4, 2022
"This course was very interesting and informative." - Marguarete, RN in Georgia
"Very informative and well written. I feel much more confident about discussing T1DM with my patients." - Ryan, OT in Tennessee
"Great course. Thank you!" - Leslie, OTA in Ohio
"Absolutely fantastic. Very thorough." - Amanda, RN in Ohio
EXCLUSIVE DISCOUNT: 50% off! Pass this course and register for your certificate to get this course for $11 instead of the regular price of $22.










Diabetes Type 1
Current Approaches in Nursing Care and Patient Management for Individuals Diagnosed with Type 1 Diabetes
Copyright © 2022 Wild Iris Medical Education, Inc. All Rights Reserved.
LEARNING OUTCOME AND OBJECTIVES: Upon completion of this course, you will be better prepared to care for patients with type 1 diabetes mellitus (T1DM). Specific learning objectives to address potential knowledge gaps include:
- Describe the impact of type 1 diabetes.
- Discuss the pathogenesis of T1DM.
- Summarize the diagnostic process for T1DM.
- Explain current management strategies for type 1 diabetes.
- Identify acute and chronic complications and interventions to prevent these complications.
TABLE OF CONTENTS
INTRODUCTION
Type 1 diabetes mellitus (T1DM) is a serious, chronic endocrine condition characterized by the body’s inability to produce insulin or to produce it in only very small amounts because of autoimmune destruction of the beta cells in the pancreas (Khardori, 2022). Without sufficient amounts of insulin, the body’s tissues do not have access to essential nutrients for fuel and storage. The entry of glucose into the cells is impaired, and blood glucose levels increase (Rebar et al., 2019).
Impact of Diabetes
Diabetes has a significant impact on the health of individuals and society. It is the seventh leading cause of death in the United States (ADA, 2022b). Important statistics related to T1DM include:
- An estimated 1.6 million Americans are living with T1DM, including about 200,000 youth (<20 years old) and 1.4 million adults (≥20 years).
- 64,000 people are diagnosed with T1DM annually in the United States.
- In the United States, there is $16 billion in T1DM-associated healthcare expenditures and lost income annually.
- Less than one third of people with T1DM consistently achieve target blood glucose levels.
(JDRF, 2020)
Pathogenesis of Type 1 Diabetes
PATHOPHYSIOLOGY
Currently, autoimmunity is considered to be the primary factor in T1DM pathophysiology. In a genetically susceptible person, a viral infection may trigger production of antibodies against a viral protein that results in an autoimmune response against antigenically similar beta cell molecules. Research shows that the prevalence of T1DM is higher in patients with other autoimmune diseases such as Graves’ disease, Addison disease, and autoimmune thyroiditis (Khardori, 2022).
In T1DM, pancreatic beta cells are destroyed or suppressed. Islet cell antibodies may be present long before symptoms are noted. By the time signs and symptoms appear, an estimated 80% of the body’s beta cells are destroyed by antibodies (Rebar et al., 2019).
RISK FACTORS
It is important for healthcare professionals to recognize persons who are at risk for developing T1DM. A number of risk factors are associated with the condition, including:
- Family history
- Genetic factors
- Viral infections (which may trigger an autoimmune response)
- Geography (people who live in Northern countries are at increased risk)
(Mayo Clinic, 2021c; MedlinePlus, n.d.)
Although overweight and obesity are risk factors typically associated with T2DM, their link to T1DM is also becoming more prevalent. Research regarding this issue is needed to provide more reliable data (Vilarrasa et al., 2021).
DIFFERENTIATING BETWEEN TYPE 1 AND TYPE 2 DIABETES
T1DM is a chronic condition in which the pancreas produces little or no insulin, most likely due to an autoimmune reaction. Various factors such as genetics and some viruses may contribute to the development of T1DM (Mayo Clinic, 2021c). In T2DM, the body is unable to properly utilize insulin, and blood glucose levels cannot be maintained at normal levels (CDC, 2021b; Mayo Clinic, 2021d).
DIAGNOSING TYPE 1 DIABETES
Diagnosis of T1DM is based on signs and symptoms and the results of diagnostic studies.
T1DM Symptoms
The hallmark clinical sign of T1DM is hyperglycemia. Additional common signs and symptoms include:
- Polyuria (the excretion of large volumes of urine) is due to a condition known as osmotic diuresis, or the build-up of substances in the kidney tubules. This increase changes the osmotic pressure within the tubules, thereby inducing water retention, which is excreted as urine. In young children, nighttime bed-wetting may occur.
- Polydipsia (excessive thirst) often accompanies polyuria. The ingestion of large volumes of liquid contributes to polyuria.
- Polyphagia (excessive hunger) is another common symptom of T1DM. Despite the consumption of large amounts of food, patients may experience weight loss. In the patient with T1DM, weight loss in the presence of normal food consumption or polyphagia is a result of both dehydration and the catabolic state.
- Fatigue and weakness are common among patients with T1DM due to catabolic muscle wasting.
- Muscle cramps can result from an imbalance in electrolytes, including sodium, chloride, and potassium.
- Gastrointestinal symptoms (e.g., nausea, abdominal pain) and neurologic changes (e.g., cerebral edema and coma) can be caused by diabetic ketoacidosis (DKA), a dangerous condition that occurs when insufficient insulin levels cause the body to break down fats instead of glucose for energy.
- Peripheral neuropathy (nerve damage occurring in the extremities) is a frequent symptom of T1DM. This is due to the build-up of sorbitol, a product of glucose conversion, in the sensory nerves of the periphery. Patients experience the onset of peripheral neuropathy first as a numbness and tingling sensation in the hands and feet.
- Blurred vision can result from glucose-induced swelling of the lens of the eye.
(Mayo Clinic, 2021c; MedlinePlus, n.d.)
Diagnostic Tests
Blood glucose tests are used for a definitive diagnosis of diabetes mellitus.
FASTING PLASMA GLUCOSE (FPG) TEST
The FPG test is a measure of the blood glucose level in an individual after a period of fasting. This method assesses the ability of the body to properly store glucose following a meal. It is performed after the patient has not eaten for at least 8 hours and is most reliable when done in the morning (Pagana et al., 2019). Diabetes is diagnosed at a fasting blood sugar of ≥126 mg/dL (ADA, 2019).
| Plasma Glucose Level (mg/dL) | Diagnosis |
|---|---|
| * Confirmed by repeating the test on a different day (ADA, 2019; Pagana et al., 2019) |
|
| <100 | Normal |
| 100–125 | Prediabetes |
| ≥126 | Diabetes* |
ORAL GLUCOSE TOLERANCE TEST (OGTT)
The OGTT measures blood glucose levels in an individual who has fasted for at least 8 hours and is administered 2 hours after that person has consumed a glucose-containing liquid (Pagana et al., 2019).
As with the FPG test, a positive diagnosis of diabetes using the OGTT must be repeated on a different day for confirmation. Diabetes is diagnosed by a 2-hour blood sugar of ≥200 mg/dL (ADA, 2019).
| 2-Hour Plasma Glucose Level (mg/dL) | Diagnosis |
|---|---|
| * Confirmed by repeating the test on a different day (ADA, 2019) |
|
| <140 | Normal |
| 140–199 | Prediabetes |
| ≥200 | Diabetes* |
GLYCOSYLATED HEMOGLOBIN (A1C) TEST
The A1C test is a measure of the percentage of hemoglobin molecules that have glucose molecules attached to them. The A1C value is indicative of the average blood glucose level in an individual over the previous two to three months. Therefore, it is considered a long-term assessment of glucose control. A1C levels <5.7% are considered normal. Diabetes is diagnosed at an A1C ≥6.5%.
| A1C Level | Diagnosis |
|---|---|
| * Confirmed by repeating the test on a different day (ADA, 2019; NIDDK, n.d.; Pagana et al., 2019) |
|
| <5.7% | Normal |
| 5.7%–6.4% | Prediabetes |
| ≥6.5% | Diabetes* |
The A1C test has several advantages when compared to the FPG and OGTT. These include:
- Greater convenience, since fasting is not necessary
- Greater preanalytical stability
- Fewer day-to-day perturbations during illness and stress
However, experts warn that these advantages may be offset because of the lower sensitivity of the A1C test, its greater cost, limited availability of A1C testing in certain portions of the developing world, and the imperfect correlation between A1C and average glucose in certain individuals (ADA, 2019; Pagana et al., 2019).
RANDOM PLASMA GLUCOSE TEST
A random plasma glucose test is an informal measure of the blood glucose level. This method is performed at random, with no fasting requirement. Using this test, a blood glucose level of ≥200 mg/dL in the presence of other symptoms may indicate that a patient has diabetes. In the case of a positive random plasma glucose test, a diagnosis of diabetes is confirmed using either an FPG, OGTT, or A1C test (ADA, 2019; Pagana et al., 2019).
DIAGNOSIS BASED ON AGE
More recent research has found that age is less a diagnostic factor than previously believed. T1DM, once considered a childhood disease, is now known to be similarly prevalent in adults. Cases are more difficult to recognize and accurately diagnose in adults because considerably more people develop T2DM rather than T1DM later in life. A significant clue to the possibility of adult T1DM is the failure of oral diabetic agents to control blood glucose. Conversely, T2DM, once considered to be a condition that only affected adults, is an increasing problem in children and adolescents throughout the world (CDC, 2021b; Mayo Clinic, 2021c, 2021d).
TESTING TO DIFFERENTIATE TYPE 1 DIABETES FROM TYPE 2 DIABETES
Several factors can be used to help differentiate between type 1 and type 2 diabetes. These include:
- Insulin levels can be measured to determine if an individual is producing insulin. Similarly, levels of C-peptide (a molecule formed when proinsulin is converted to insulin) are also measured to determine whether the patient’s body is producing insulin. An insulin level of <5 µU/mL or a C-peptide test ≤0.6 mg/mL is suggestive of T1DM.
- Because T1DM is considered an autoimmune disease, further blood work can be used to test for the presence of autoantibodies. Pancreatic islet cell antibodies are present in nearly 85% of patients with T1DM.
- A urinalysis may be performed to assay for the presence of ketones, the acidic byproduct of the breakdown of fat molecules. Accumulation of ketones can result in diabetic ketoacidosis (DKA). This condition rarely occurs in patients with T2DM, and therefore their presence in urine is considered indicative of T1DM.
(ADA, 2022a; Rebar et al., 2019)
MANAGEMENT OF TYPE 1 DIABETES
The American Diabetes Association Standards of Medical Care in Diabetes (2022a) notes that diabetes is a “complex, chronic illness requiring continuous medical care with multifactorial risk-reduction strategies beyond glycemic control. Ongoing diabetes self-management education and support are critical to preventing acute complications and reducing the risk of long-term complications. Significant evidence exists that supports a range of interventions to improve diabetes outcomes.”
The ADA recommends the Chronic Care Model (CCM) to improve compliance with treatment standards. The CCM includes six core elements to optimize patient care. These are:
- Delivery system design (moving from a reactive to a proactive care delivery system in which planned visits are coordinated through a team-based approach)
- Self-management support
- Decision support (basing care on evidence-based, effective care guidelines)
- Clinical information systems (using registries that can provide patient-specific and population-based support to the care team)
- Community resources and policies (identifying or developing resources to support healthy lifestyles)
- Health systems (to create a quality-oriented culture)
Patient and Family Teaching, Self-Management, and Follow-Up
The ADA publishes recommendations for diabetes self-management education and support (DSMES). Self-management education and support should be patient-centered and may be offered in group or individual settings. The entire healthcare team should be part of these education efforts.
The goal of DSMES is to “facilitate the knowledge, decision-making, and skills mastery necessary for optimal diabetes self-care and incorporate needs, goals, and the life experiences of the person with diabetes” (ADA, 2022a). Data from research studies show that DSMES is associated with improved diabetes knowledge and self-care behaviors, lower A1C, lower self-reported weight, and improved quality of life.
DSMES includes the following education topics:
- Explanation of T1DM
- Carbohydrate counting and the patient’s diet
- How to monitor and maintain blood glucose levels
- How to administer insulin
- Managing illness and infections
- Scheduling and attending regular physical exams with clinicians
- A1C testing
- What is involved in staying healthy
- Managing diabetes in school or at work
- Preventing long-term complications
(ADA, 2022a)
It is not always easy to keep in-person healthcare appointments. In such cases, digital coaching and digital self-management interventions can be effective ways to offer DSMES to patients and families (ADA, 2022a). The use of technology provides a variety of options to meet the needs of patients.
Multidisciplinary Approach to Care
Research findings show that DSMES is most effective when provided by a multidisciplinary team. Such teams typically consist of nurses, physicians, dietitians, pharmacists, mental health specialists, physical therapists, occupational therapists, exercise physiologists, diabetes educators, and community health workers.
Multidisciplinary care includes:
- A team approach in which experts, patients, and families deal with both the treatment plans and delivery of care and the psychosocial aspects of care
- Regular communication with team members
- Access to a full range of therapeutic options, irrespective of geographical remoteness and rural or urban healthcare service
- Inclusion of patients and families in the development of their plan of care and in receiving timely and appropriate information
Documented benefits of a multidisciplinary approach include:
- Access to multiple experts for enhanced patient education
- Better glycemic control
- Increased patient follow-up
- Greater patient satisfaction
- Lower risk for diabetes complications
- Improved quality of life
- Reduced hospitalizations
- Decreased healthcare costs
(CDC, 2021a)
One of the challenges of a multidisciplinary team approach is having all team members work together (with patients and families) to coordinate and deliver care. Some team members may think that a team approach simply means that each discipline provides services as they are accustomed to doing and simply document progress in multidisciplinary notes. A multidisciplinary approach to coordinated care, however, is a collaborative process during which treatment plans and care delivery become a shared responsibility. Each member of the team treats all other members of the team with respect (Saini, 2022).
Although team members provide services in which they are experts, all members must come together (in person or virtually) regularly in order to develop, implement, and evaluate the effectiveness of patient care services. It is critical to remember that patients and families must be included as equal members of the team and that their input must be respected (CDC, 2021a; Saini, 2022).
TEACHING CHILDREN
When teaching children about their T1DM, it is important to talk to them in age-appropriate ways and to always be honest. Children need to know that getting diabetes is not their fault, that it is not going to go away, and that it is okay to feel sad or upset.
Some tips for talking to a child based on age include:
- Infants and toddlers. At this age children do not understand the need for medications, injections, etc. The child should be comforted by using a gentle tone and calming words when giving injections or finger sticks. The goal is to make these activities part of the child’s daily, anticipated routine.
- Preschoolers. Simple terms should be used to describe diabetes care. Let the child have some sense of control over their care, such as choosing a snack from recommended options or choosing where to receive injections. Participation is important.
- Grade school through middle school. Children at this age should be helped to assume some responsibility for their care, but parental supervision is still needed. Parents should start with one task and gradually give the child more responsibility. The diabetic healthcare team can help identify age-appropriate tasks for the child.
- Teens. Teens should be encouraged to discuss how they feel about having diabetes, especially at school and in social situations. Teens very much want to “fit in” with their peers. These feelings may lead them to experiment with substances such as alcohol and drugs, which can affect blood glucose. It is important to talk about these temptations. Teens should be encouraged to assume responsibility for their care while being willing to accept guidance and support from parents and other influential adults.
(KidsHealth, 2022)
Diet Planning for Patients with Diabetes
Diet is one of the first and major steps addressed when developing a strategy to manage T1DM since maintaining a healthy diet is a crucial part of managing blood glucose levels.
Healthcare professionals may think that dietary discussions are the sole responsibility of the certified dietitian. However, patients may ask questions of whomever they are interacting with at the time. Thus, all members of the healthcare team must be familiar with dietary planning principles, for example, which types of food are high in fiber. To be able to provide answers (including acknowledging that the answer is not known) helps to enhance the patient’s confidence in the team. Specific dietary questions may always be referred to the dietitians who are working with patients (ADA, 2022a).
Contrary to general belief, there is not a specific “diabetes diet.” Individual patients’ preferred eating habits and lifestyle must be taken into careful consideration when designing their diet plan. This plan should include a recommended daily caloric intake based on the age and physical activity level of the patient as well as guidance for how these calories should be divided throughout the day.
RECOMMENDED FOODS
The key to healthy eating with diabetes is to eat a variety of healthy foods from all food groups. Foods and drinks with added fats, sugars, and sodium should be avoided (Mayo Clinic, 2021a).
Healthy Carbohydrates
Patients should focus on eating healthy carbohydrates, including:
- Fruits
- Vegetables
- Whole grains
- Legumes
- Low-fat dairy products
(Mayo Clinic, 2021a)
Fiber-Rich Foods
Dietary fiber moderates food digestion and helps to control glucose levels. High fiber foods include:
- Vegetables
- Fruits
- Nuts
- Legumes
- Whole grains
(Mayo Clinic, 2021a)
Heart-Healthy Fish
It is recommended that heart-healthy fish be consumed at least twice a week. Examples include salmon, tuna, and sardines, which are rich in omega-3 fatty acids. Fried fish and fish containing high levels of mercury (e.g., king mackerel) are to be avoided (Mayo Clinic, 2021a).
“Good” Fats
Foods that contain monosaturated and polyunsaturated fats are the so-called good fats and include avocados, nuts, and canola, olive, or peanut oils. The amount of these fats consumed should be moderated. All fats are typically high in calories (Mayo Clinic, 2021a).
Foods to Be Avoided
There are several types of food that persons with diabetes should avoid. Diabetes increases the risk of stroke and heart disease by facilitating the development of plaque buildup in the arteries. Foods that contain the following components can interfere with achieving the best possible patient outcomes:
- Saturated fats: High-fat dairy products and animal proteins such as butter, beef, hot dogs, bacon, and coconut and palm kernel oils
- Trans fats: Found in processed snacks, baked goods, shortening, and stick margarines
- Cholesterol: Abundant in egg yolks, liver, and other types of organ meats; should be limited to <200 mg per day
(Mayo Clinic, 2021a)
NUTRIENT AMOUNTS
A dietary plan is developed based on the individual needs of each patient. There are typically two meal plan methods to help determine nutrient consumption: the plate method and carbohydrate counting (ADA, 2022a; Mayo Clinic, 2021a).
Plate Method
The plate method helps patients to control portion sizes. Recommendations include:
- Using a 9-inch (i.e., smaller) plate
- Filling one half of the plate with nonstarchy vegetables (e.g., spinach, carrots)
- Filling one quarter of the plate with protein (e.g., tuna, lean chicken)
- Filling the final one quarter of the plate with whole-grains (e.g., brown rice, starchy vegetables)
- Including “good” fats such as nuts or avocados in small amounts
- Adding a serving of fruit or dairy and water or unsweetened coffee or tea
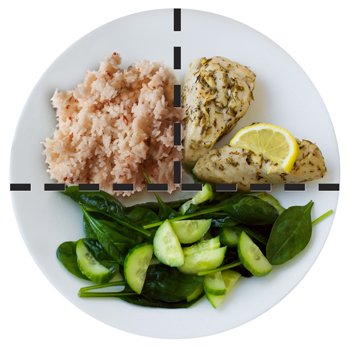
The plate method shows the relative portions of each type of food. (Source: NIDDK.)
JUDGING PORTION SIZES
Every-day objects can help patients and families judge portion sizes. These include:
- 1 serving of meat or poultry is the size of a deck of cards.
- 1 three-ounce serving of fish is the size of a checkbook.
- 1 serving of cheese is the size of six pairs of dice.
- 1/2 cup of cooked rice or pasta is the size of rounded handful or a tennis ball.
- 2 tablespoons of peanut butter is the size of a ping-pong ball.
(MedlinePlus, 2020)
Carbohydrate Counting
Carbohydrate counting involves keeping track of the amount of carbohydrates eaten and drunk each day. Counting carbs can help patients know the amount of insulin to take. Most carbohydrates come from starches, fruits, milk, and sweets. Carbohydrates from added sugars or refined grains (e.g., white bread and white rice) should be limited. Instead, fruit, vegetables, whole grains, beans, and low-fat or nonfat milk are recommended (NIDDK, 2022).
Physical Activity
Regular exercise is critical to managing diabetes. Research findings show that exercise may lower blood pressure and blood glucose levels, improve mood, and improve blood flow. Exercise should be undertaken only with approval of the patient’s primary care provider and under the supervision of a physical therapist or exercise physiologist, and may include strengthening exercises such as weight training and stretching exercises such as yoga (ADA, 2022a; Mayo Clinic, 2021b).
Recommendations for adults include:
- Aerobic activity: Over the course of a week, 150 minutes of moderate aerobic activity or 75 minutes of vigorous aerobic activity, or a combination of both
- Strength training: Strength training exercises for all major muscle groups at least two times a week
(Mayo Clinic, 2021b)
Managing Blood Glucose Levels
It is important for patients with T1DM to maintain normal blood glucose levels. Achieving and maintaining glycemic control is associated with reductions in the frequency and severity of diabetes-related complications. Target blood glucose levels are:
- 80–130 mg/dL before meals
- <180 mg/dL two hours after meals
It is important to acknowledge that target goals vary depending on age and personal health. Some people will have slightly higher blood sugar goals, including people who:
- Are age 60 and older
- Have other medical conditions, such as heart, lung, or kidney disease
- Have a reduced ability to sense low blood sugar levels (hypoglycemia unawareness)
(Mayo Clinic, 2022a)
CONTINUOUS GLUCOSE MONITORING (CGM)
Patients with T1DM are educated to frequently monitor their blood glucose levels, as this can be used to determine whether their disease is being properly treated. Self-monitoring of blood glucose allows patients to evaluate their individual response to therapy and assess whether glycemic targets are being achieved on a daily basis. Research indicates that CGM helps to reduce hypoglycemia and improve glucose control (Lakhanigam, 2019).
CGM automatically tracks blood glucose levels every few minutes, 24 hours per day. CGM works via a tiny sensor inserted under the skin, usually on the abdomen or arm. The sensor measures the interstitial glucose level, and a transmitter wirelessly sends the information to a monitor. This monitor may be part of an insulin pump or separate device that can be carried in a pocket or purse. An alarm sounds if blood glucose levels are increasing or decreasing too rapidly.
Sensors are typically worn for a one or two weeks before needing to be changed. The newest type of CGM monitor has an implanted sensor and can determine blood glucose levels for up to three months. The transmitter sends blood glucose information from the sensor to a smartphone or smartwatch app. Such computerized CGMs provide the most accurate and precise measure of the amount of glucose circulating within the blood at a particular time.
Most devices still require finger-stick checks in order to calibrate the machine (Mayo Clinic, 2022a).
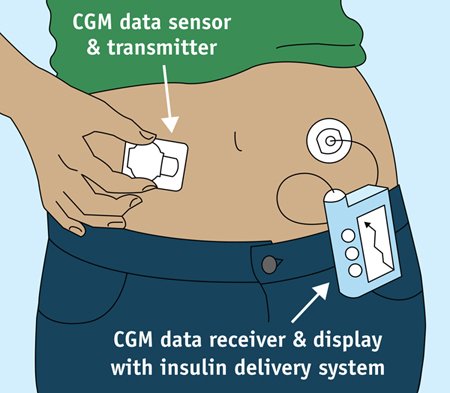
Continuous glucose monitoring and insulin delivery system. (Source: NIDDK.)
MEDICATIONS AND CGM ACCURACY
Medications such as acetaminophen, albuterol, and lisinopril may interfere with CGM reading accuracy. This is especially true of older CGM models. Healthcare providers should be consulted about any medications the patient is taking and how they may affect glucose readings (Mayo Clinic, 2022a).
A1C TESTING
The A1C test is a measure of the percentage of hemoglobin molecules that have glucose molecules attached. The A1C level is reflective of the average blood glucose level in an individual over the previous two to three months and is considered a long-term assessment of glucose control (Dansinger, 2020).
The 2022 ADA recommendations include the following A1C goals for adults with diabetes:
- A reasonable A1C goal for many nonpregnant adults is <7% (53 mmol/mol).
- Providers might reasonably suggest more stringent A1C goals (such as <6.5%, or 48 mmol/mol) for select individual patients if this can be achieved without significant hypoglycemia or other adverse effects of treatment.
- Less stringent A1C goals (such as <8%, or 64 mmol/mol) may be appropriate for patients with a history of severe hypoglycemia, limited life expectancy, advanced microvascular or macrovascular complications, extensive comorbid conditions, or long-standing diabetes in whom the goal is difficult to achieve despite diabetes self-management, education, appropriate glucose monitoring, and effective doses of multiple glucose-lowering agents including insulin.
- Glycemic targets should be reassessed over time based on ADA criteria.
ESTIMATED AVERAGE GLUCOSE (eAG)
Estimated average glucose is a method for understanding the management of diabetes. The eAG is determined by converting the A1C percentage to mg/dL units. Because these units are the same as those used on blood glucose meters, they are considered to be more familiar to patients with diabetes. Therefore, providing the A1C percentage in these units may help patients to better understand how effectively their T1DM is being controlled (Gilles, 2022).
DIABETES AND TECHNOLOGY
Technological devices provide a variety of hardware and software that may help with the management of diabetes (ADA, 2022a). Choosing the type of technology that is best suited to each patient is very individualized. The “Resources” list at the end of this course provides links to help in identifying available technology and determining what is best for each patient.
Insulin Therapy
Because type 1 diabetes is a disease caused by a loss of the ability to produce insulin, the primary treatment is insulin therapy. In addition, other medications may be prescribed to work in conjunction with insulin in an effort to reduce hyperglycemia.
The 2022 ADA recommendations regarding pharmacologic therapy for T1DM state:
- Most individuals with type 1 diabetes should be treated with multiple daily injections of prandial and basal insulin, or continuous subcutaneous insulin infusion.
- Most individuals with type 1 diabetes should use rapid-acting insulin analogs to reduce hypoglycemia risk.
- Individuals with type 1 diabetes should receive education on how to match mealtime insulin doses to carbohydrate intake, fat and protein content, and anticipated physical activity.
INSULIN ADMINISTRATION
The way insulin is administered depends on the patient’s lifestyle, insurance plan, and preferences. Most people with diabetes administer insulin via a needle and syringe, insulin pen, or insulin pump.
Needle and Syringe
Insulin is administered as a subcutaneous injection. The drug works most rapidly when it is injected into the abdomen. Repeated injections into the same spot could cause tissue to harden, making it difficult to inject into that area over time. Insulin may also be injected into the thigh, buttocks, or upper arm (NIDDK, 2022).
Insulin Pen
Insulin pens allow the delivery of insulin in a simpler, more accurate, and more convenient manner than vial and syringe administration. Several brands and models of insulin pens are available. Most insulin pens belong to one of two categories (ADA, n.d.):
- Disposable pens contain prefilled insulin cartridges and are thrown away after the insulin cartridge is empty or the pen has been in use for 28 or 32 days (depending on insulin type).
- Reusable pens work with insulin cartridges that can be loaded into the pen and then tossed away once the insulin is used, leaving the pen ready for the next cartridge. Different types of pens work with certain types of insulin, so pens that are compatible with the type of insulin being administered must be purchased.
Insulin Pumps
An insulin pump delivers insulin through a thin plastic tube placed semipermanently under the skin, typically in the stomach area or back of the upper arm. (See illustration earlier in this course.) The pump is about the size of a small cell phone and provides a minimal (basal) amount of insulin throughout the day and night. The pump can be calibrated to keep blood glucose levels within the desired target range throughout the day. Patents can also use the pump to administer a bolus as needed after a meal or snack, or less insulin when very active. An insulin pump allows the patient greater flexibility with meals, exercise, and daily activities (CDC, 2021c).
Inhaled Insulin
Inhaled insulin is administered via an oral inhaler that delivers ultra-rapid-acting insulin at the beginning of meals. Inhaled insulin is used in conjunction with injectable, long-acting insulin. There are several advantages to using insulin inhalers. Onset of action is rapid, they can be used at the start of meals, they may lower the risk of hypoglycemia, and they may lead to less weight gain. Disadvantages include the potential for mild or severe coughing, greater expense, requirement for continued injections or pump for basal insulin, and less-precise dosing (CDC, 2021c).
CLOSED-LOOP INSULIN DELIVERY SYSTEMS
The FDA has approved hybrid closed-loop pump systems (also called automated insulin delivery [AID] systems). The safety and efficacy of these systems has been supported in the literature for adolescents and adults with type 1 diabetes.
A hybrid closed-loop system combines a continuous glucose monitoring (CGM) sensor with an insulin pump in order to automate insulin delivery. This system is sometimes referred to as an artificial pancreas. Its purpose is to replicate how a pancreas would respond to changes in blood glucose levels.
Advanced features of this hybrid closed-loop system include predictive algorithms that provide parameters to the pump on when to administer or stop insulin based on real-time glucose readings. This is combined with settings that allow the user to also administer insulin (e.g., mealtime boluses) when needed (Pinsker, 2022).
TYPES OF INSULIN
Types of insulin are categorized based on their time of onset, peak, and duration of action. Rapid, short, intermediate, and long-acting insulin preparations are available for use in the United States. Recombinant human insulin is now used almost exclusively, although commercially prepared mixtures of insulin are also available (ADA, 2022a; Khardori, 2022).
Insulin replacement regimens typically consist of basal insulin, mealtime insulin, and correction insulin. Basal insulin includes NPH insulin, long-acting insulin analogs, and continuous delivery of rapid-acting insulin via an insulin pump (ADA, 2022a).
The following table describes various types of insulin, including their onset, peak, and duration.
| Name | Onset (hours) |
Peak (hours) |
Duration (hours) |
|---|---|---|---|
| (Comerford & Durkin, 2022; Khardori, 2022) | |||
| Rapid- and Short-Acting | |||
| Glulisine insulin | 0.25 | 0.5–1.5 | 3–5 |
| Lispro insulin | 0.25 | 1–3 | 1–5 |
| Aspart insulin | 0.25 | 1–3 | 1–5 |
| Regular insulin | 0.5–1 | 2.5–5 | 4–12 |
| Intermediate-Acting | |||
| Neutral protamine Hagedorn (NPH) | 1–2 | 4–12 | 12–18 |
| Long-Acting | |||
| Insulin detemir (Levemir) | 1 | stable levels (no peak) | 24 |
| Insulin glargine (Lantus, Toujeo) | 1–2 | stable levels (no peak) | 24 |
MEDICATIONS THAT MAY REQUIRE INSULIN ADJUSTMENTS
Patients who are taking the following medications may require an adjustment to their insulin therapy:
- Atypical antipsychotics: May cause weight gain and insulin resistance
- Corticosteroids: May cause insulin resistance, sensitivity to glucose, and inability to release insulin in other tissues
- Niacin: May slightly increase glucose levels
- Beta blockers: May impair insulin release by nonselective beta blockers
- Thiazide diuretics: May have a weak inhibitory effect on insulin release from beta cells
- Fluoroquinolones: May cause severe blood sugar swings
- Immunosuppressive agents: May decrease insulin secretion, have a direct toxic effect on cells, and/or increase insulin resistance
- Protease inhibitors: May predispose people to diabetes by increasing insulin resistance
- Pentamidine: May cause transient hyperinsulinemia associated with hypoglycemia and beta cell failure
- Alcohol: May block hepatic glucose production, which can lead to hypoglycemia
(Waleed, 2019)
AMYLIN THERAPY
Amylin analogues (or agonists) are injectable drugs that mimic the functions of the hormone amylin. Amylin is an amino acid polypeptide hormone produced by the pancreas and released at the same time as insulin but in much smaller amounts (Diabetes.co.uk, 2022).
Currently, the amylin analog pramlintide (Symlin) is FDA approved. It is an injected medication for people with both T1DM and T2DM. Pramlintide lowers glucagon during a meal, slows food emptying from the stomach, and diminishes appetite. Side effects include nausea, vomiting, headache, and low blood sugar. These side effects occur primarily at the start of pramlintide therapy. Thus, the starting dose is small to allow for the body to adjust to the medication (UCSF, 2022).
Transplantation Procedures
Pancreatic and islet cell transplantation are procedures that involve replacing a diseased pancreas and islet cells with healthy ones in cases of uncontrollable diabetes.
Candidates for islet cell transplantation include people with T1DM who:
- Are ages 18 to 65 years
- Have blood glucose levels that are difficult to manage
- Have poorly controlled T1DM with episodes of severe hypoglycemia and hypoglycemia unawareness
- May need or have already had a kidney transplant
- Are pregnant, trying to become pregnant, or nursing a baby because of the effect of immunosuppressant drugs on a baby in utero or who is ingesting breast milk (women of childbearing age must agree to use contraception)
(Cervoni, 2022)
Candidates for pancreas transplant are persons ages 18 to 55 with a body mass index <32 and who:
- Typically have T1DM in conjunction with kidney damage, nerve damage, eye problems, or other complications of diabetes
- Typically have diabetes that is out of control
(Johns Hopkins Medicine, 2022; University Hospitals, n.d.)
ISLET CELL TRANSPLANTATION
Islet cell transplantation involves taking islet cells from the pancreas of an organ donor and transplanting these cells into a person who has T1DM. It is a relatively simple nonsurgical procedure that takes about an hour. The patient is awake throughout the procedure. A catheter is inserted into the portal vein that leads to the liver. Purified islets flow from an infusion bag through the portal vein and are dispersed throughout the liver. The transplanted cells are able to establish a new blood supply and start to produce insulin (Diabetes Research Institute, 2022).
PANCREAS TRANSPLANTATION
During a pancreas transplant, a healthy pancreas from a deceased donor is received by the patient. The patient’s own pancreas is typically left in place to facilitate digestion. The new pancreas is usually connected to the patient’s intestines so that digestive juices can drain. A functioning transplanted pancreas means that insulin therapy is no longer needed (Johns Hopkins Medicine, 2022).
Patients with T1DM who are candidates for a pancreas transplantation are typically those who have developed kidney damage, nerve damage, eye issues, or another complication of the disease and/or whose diabetes is out of control even with medical intervention.
There are several types of pancreas transplantation procedures, including:
- Pancreas transplant alone: Patients without kidney disease may be candidates for a pancreas transplant.
- Combined kidney-pancreas transplant: This procedure is often performed for patients with diabetes who have, or are at risk of, kidney failure. Simultaneous kidney-pancreas transplant tends to have a lesser likelihood of organ rejection.
- Pancreas after kidney transplant: For patients who are facing a long wait for a pancreas donor, a kidney transplant may be recommended first.
Patients who receive transplants must take immunosuppressant drugs and carefully manage blood glucose levels for the rest of their lives. The prognosis for those who receive a pancreas transplant is quite good (Mayo Clinic, 2022b; Johns Hopkins Medicine, 2022).
Contraindications for pancreatic transplantation include:
- Malignancy within the past two years
- Inadequate social or family support
- Significant noncompliance with treatment plan
- Central vascular disease
- Significant coronary artery disease
- Severe malnutrition
(UNC School of Medicine, n.d.)
PATIENT NONADHERENCE TO THERAPY
The issue of nonadherence to diabetes management is closely linked to the development of diabetes-related complications. In fact, nonadherence is one of the leading causes of mortality and morbidity in patients who have diabetes (Boshe et al., 2021).
Research indicates that nonadherence is a problem affecting patients with a multitude of diseases, not just diabetes. For example, an estimated 125,000 people with treatable illnesses die every year in the United States because of failure to take their medication as ordered (Torrey, 2021).
Common reasons for nonadherence include:
- Denial of the problem or denial of the seriousness of the problem
- Treatment cost
- Complexity of the treatment regimen/inability to follow the treatment regimen because of confusion or other issues
- Side effects of treatment
- Apathy towards the treatment
- Previous negative experience with treatment plans
(Torrey, 2020)
CASE
A 14-year-old boy, diagnosed with T1DM one year ago, has been hospitalized three times in the intervening months for DKA. His blood sugars have fluctuated greatly, and he has reported feeling shaky in the middle of the night on occasion. He does not like to check his blood sugar and often finds himself feeling “sick” between meals. The patient complains that checking his blood sugar at school makes him feel “weird,” and he “just wants to be a normal kid.”
Social service interviews with the family reveal that the boy was also diagnosed with depression six weeks ago but that he does not routinely take his antidepressant medication. He also does not take his insulin without close supervision by his parents, who report that they often have to argue with him about his need to take his insulin doses. It had been suggested that the patient attend a summer camp for youth with diabetes, where he could meet other teenagers coping with the disease, but so far he has refused to go.
The patient is currently admitted for another episode of DKA. He states that he hates being diabetic, is very depressed about it, and is considering trying to kill himself because of these depressed feelings. After he is medically stabilized following the DKA episode, the patient is transferred to the psychiatric ward of the hospital for observation and treatment for suicidality and severe depression.
Discussion
Depression can be a reaction to stress and changes in routine that occur because of the T1DM diagnosis and the demands and responsibilities required by its treatment. Apathy associated with depression can interfere with a patient’s ability to handle these demands and responsibilities. Because of the lifelong nature of T1DM, patients with the disease must contend with these demands and responsibilities on an ongoing basis, which may require long-term emotional support in the form of personal and family counseling to promote optimal motivation and adherence to their plan of care.
After his initial psychiatric hospitalization and stabilization for depression, a teenaged patient such as this one who is having trouble accepting his diagnosis may benefit from individual and family counseling, from being involved in a peer support group, and from short- or long-term antidepressant medication therapy. In addition, the patient and his family may benefit from the support of agencies (such as Children with Diabetes) that are dedicated to assisting children and teens with the challenges that accompany the disease. (See also “Resources” at the end of this course.)
PREVENTING AND TREATING COMPLICATIONS
The potential for both acute and chronic complications is a serious consequence for those with T1DM. Preventing or delaying such complications is an essential part of the management of the disease (Rebar et al., 2019).
Acute Complications
Acute complications are generally described as hypoglycemia, hyperglycemia, and diabetic ketoacidosis (DKA). Left untreated, such complications can have serious ramifications.
HYPOGLYCEMIA
Hypoglycemia is common among persons with T1DM. It occurs when the blood glucose level drops below what is considered healthy for the individual patient. For many patients, this is a blood glucose reading of <70 mg/dL (NIDDK, 2021).
Preventing Hypoglycemia
The best way to “treat” hypoglycemia is to prevent it as much as possible. Patients and families should be educated regarding:
- Meticulously monitoring blood glucose levels
- Ensuring that meal plans include meals, snacks, and beverages with enough carbohydrates to maintain blood glucose within the target range
- Carrying a source of fast-acting carbohydrates at all times
- Monitoring blood glucose before, during, and after physical activity, and changing medication dose and/or carbohydrate intake to prevent low blood glucose
(NIDDK, 2021)
Recognizing and Treating Hypoglycemia
Hypoglycemia can have an abrupt onset and, initially, mild symptoms. However, recognition of even mild symptoms requires immediate intervention (see box below).
SYMPTOMS OF HYPOGLYCEMIA
- Weakness
- Fatigue
- Hunger
- Shakiness
- Nervousness
- Sweating
- Dizziness
- Light-headedness
- Sleepiness
- Confusion
- Difficulty speaking
- Anxiety
If hypoglycemia occurs during sleep, patients may cry out or have nightmares; sweat excessively; and feel tired, irritable, or confused upon awakening.
(Comerford & Durkin, 2022; Rebar et al, 2019; NIDDK, 2021)
If hypoglycemia symptoms occur, blood glucose levels are to be checked immediately. If results are below target or <70mg/dL, patients are instructed to:
- Immediately eat or drink 15–20 grams of glucose or carbohydrates (e.g., 4 ounces of fruit juice, not low-calorie or reduced-sugar). If kidney disease is present, avoid orange juice since it is high in potassium. Four glucose tablets or one tube of glucose gel is also appropriate.
- If after 15 minutes the blood glucose level is still low, consume another 15–20 grams of glucose or carbohydrates.
- Check blood glucose levels every 15 minutes and consume glucose or carbohydrates again until glucose levels are within the healthy range.
- If the next meal is more than 1 hour away, have a snack to keep blood glucose levels within the target range.
CASE
Michael, a 26-year-old male, has had T1DM since middle school. With very few episodes of hypoglycemia in the last five years, he feels very confident in his ability to manage his disease.
One day, he follows his usual morning routine of wake-up CBG and insulin. When he arrives at work, where he is the manager of all the concession booths at a large amusement park, he is immediately informed of a power failure that has affected all the food coolers in the booths. In the rush of responding to this crisis, he forgets about his usual practice of eating a breakfast bar.
Thirty minutes later, Michael’s supervisor notices that he is shaky, sweating, and disoriented. Knowing about Michael’s diabetes, the supervisor takes him to the park’s first aid station, where his CBG tests as 46 mg/dL. While waiting for an ambulance to arrive, the nurse on duty coaches Michael in drinking a sweetened electrolyte replacement solution. The EMS team arrives and administers glucose gel orally and monitors the patient’s CBG until he meets discharge criteria.
Once he is stable, Michael returns to work. Considering the seriousness of this “close call,” he resolves to rethink his self-care plan. He pre-positions energy bars approved by his diabetes educator in his desk, car, and pouch he wears at work.
Knowing that there are several other staff members with diabetes working at the park, as well as likely visitors who may have the same problem, the nurse in charge of first aid takes the EMS team’s recommendation to stock glucose gel and the solution formulation as part of the station’s supplies.
Discussion
Patients with type 1 diabetes who have not experienced an episode of hypoglycemia in some time may become complacent with their self-management plan. In this case, the patient’s situation was aggravated by the additional stress and physical activity prompted by the power failure. He lost track of the elapsed time since he had taken his insulin and the additional demands being placed on his body. Had he been working alone, he might not have been found and helped in time.
HYPERGLYCEMIA
Hyperglycemia is generally defined as a blood glucose level greater than 125 mg/dL while fasting. Additionally:
- A person has impaired glucose tolerance, or pre-diabetes, with a fasting blood glucose of 100–125 mg/dL.
- A person has hyperglycemia if their blood glucose is >180 mg/dL one to two hours after eating.
(Cleveland Clinic, 2020)
Preventing Hyperglycemia
Ways to prevent hyperglycemia include:
- Exercising regularly
- Adhering to a meal plan and treatment regimen
- Maintaining a healthy weight
- Not smoking
- Limiting alcohol intake
(Cleveland Clinic, 2020)
Recognizing and Treating Hyperglycemia
SYMPTOMS OF HYPERGLYCEMIA
- Increased thirst or hunger
- Blurred vision
- Frequent urination
- Headache
- Fatigue
- Slow-healing infections
- Weight loss
(Cleveland Clinic, 2020)
Emergency treatment for severe hyperglycemia include fluid replacement, electrolyte replacement, and insulin therapy (Mayo Clinic, 2020). More generally, hyperglycemia is treated by changes in exercise, diet, and/or alterations to the patient’s insulin regimen (Ambardekar, 2021). Untreated hyperglycemia can lead to the development of ketoacidosis (see below).
DIABETIC KETOACIDOSIS (DKA)
DKA is a serious acute complication that may lead to cerebral edema, diabetic coma, and if not treated, death. This condition occurs when insufficient insulin levels cause the body to break down fats instead of glucose for energy. DKA develops quickly, often in only a few hours. Although DKA may occur in anyone with diabetes, it is far more common in patients with T1DM compared to those with T2DM (Rebar et al., 2019).
Common causes of DKA include:
- Infection
- Illness (e.g., pneumonia or influenza)
- Missed insulin dose(s)
- Inadequate insulin dosage
- Stress
- Alcohol and/or drug abuse
- Surgery
- Trauma
- Heart attack
(Rebar et al., 2019; Mayo Clinic, 2021c)
Preventing DKA
In order to prevent DKA, patients are advised to:
- Check blood glucose levels frequently
- Take insulin and/or medication as prescribed
- Check blood or urine for ketones
- Check insulin pumps for issues such as kinked cannula or a disconnected site/tubing
- Have a sick-day plan
- Seek out information/education regarding DKA
- Seek support from family, friends, and the multidisciplinary team
(Cleveland Clinic, 2021)
Recognizing and Treating DKA
SYMPTOMS OF DKA
- Thirst
- Dry mouth
- Frequent urination
- High blood glucose levels
- Nausea and vomiting
- Abdominal pain
- Kussmaul breathing
- Fatigue
- Dry or flushed skin
- Confusion
- Fruity breath odor
(Mayo Clinic, 2021c; Rebar et al., 2019)
DKA is typically diagnosed if these four conditions exist:
- Blood glucose level >250 mg/dL
- pH <7.3 (acidosis)
- Presence of ketones in urine and/or blood
- Serum bicarbonate level <18 m/Eq per L
(Cleveland Clinic, 2021)
Emergency treatment of DKA includes:
- Fluid replacement either by mouth or intravenously
- Electrolyte replacement (e.g., calcium, potassium)
- Insulin therapy administered intravenously
(Mayo Clinic, 2021c; Rebar et al., 2019)
THE “KETO” DIET AND DIABETES
There is no definitive consensus as to whether or not a ketosis-inducing diet is an effective and safe adjunctive therapy to insulin in T1DM. However, research indicates that:
- Ketogenic diets are high in fat, moderate in protein, and low in carbohydrate, and should be used by people with T1DM only with careful supervision.
- Ketogenic diets have been reported to improve hemoglobin A1C and glycemic variability in patients with type 1 diabetes and may improve biochemical and physical markers of cardiovascular risk.
- Safety concerns of a ketogenic diet include the risks of dyslipidemia, DKA, and hypoglycemia.
- Insulin therapy usually requires adjustment when starting a ketogenic diet, and patients should be closely monitored.
(Buehler et al., 2021)
Chronic Complications
Diabetes can cause a variety of complications that can affect almost every body system. It is important that healthcare professionals work closely with patients and their families to prevent or minimize the effects of such complications.
CARDIOVASCULAR CONDITIONS
Patients with T1DM have an increased risk for a number of cardiovascular complications, including heart disease, stroke, and hypertension. Because of the seriousness of cardiovascular complications, patients with T1DM are counseled to follow their recommended diet; perform regular aerobic exercise; and undergo regular screening for risk factors, signs, and symptoms of cardiac disease as means of preventing cardiovascular conditions (ADA, 2022a).
Among the cardiovascular complications, hypertension (sustained BP ≥140) is common among patients with either T1DM or T2DM. Thus, blood pressure (BP) control is imperative in the patient with diabetes. BP should be measured at every routine clinical visit, and patients should monitor their BP at home (ADA, 2022a).
For patients with blood pressure >120/80 mmHg, lifestyle intervention consists of weight loss when indicated, a Dietary Approaches to Stop Hypertension (DASH)–style diet including reducing sodium and increasing potassium intake; moderation of alcohol intake; and increased physical activity (ADA, 2022a).
DIABETIC NEUROPATHY AND FOOT COMPLICATIONS
Diabetic neuropathy is a type of nerve damage associated with diabetes. Peripheral neuropathy, the most common type of diabetic neuropathy, affects the feet and legs first and progresses to the hands and arms. Because peripheral neuropathy is a common complication for patients with diabetes, it should be screened for at each clinic visit. Tests commonly used to diagnose neuropathy include filament testing, quantitative sensory testing, nerve conduction studies, electromyography, and autonomic testing. Prevention measures include consistent blood sugar management and a healthy lifestyle (Mayo Clinic, 2022c).
SYMPTOMS OF DIABETIC PERIPHERAL NEUROPATHY
Warning signs of diabetic peripheral neuropathy, often worse at night, may include:
- Tingling or burning feelings, usually in the hands and feet
- Numbness or reduced sensitivity to pain or temperature changes, usually in the hands and feet
- Sharp pains or cramps
- Muscle weakness
- Extreme sensitivity to touch
- Serious foot problems, such as ulcers, infections, and bone and joint damage
(Mayo Clinic, 2022c)
A diabetic foot ulcer (DFU) is the most frequently occurring complication associated with diabetes, typically the result of diabetic peripheral neuropathy. Diabetic foot ulcers are complex, chronic wounds that are often disabling and greatly impact the morbidity and mortality of patients. Patients who develop a DFU are at higher risk of early death, heart attack, and fatal stroke than people with diabetes who do not develop diabetic foot ulcers. Data shows that 40%–70% of those with a DFU will end up with a lower limb amputation (Cheng et al., 2021).
FOOT CARE
Diabetic foot care at all stages, both preventive and in treating a diabetic foot ulcer, is a critical component of patient care. Prevention measures include regular foot checks, a thorough foot exam at least once a year, and good foot care, including:
- Daily check for blisters, cuts, bruises, swelling, etc.
- Keeping feet clean and dry
- Moisturizing to prevent cracking
- Trimming toenails carefully
- Wearing clean, dry socks
- Wearing cushioned, well-fitted, closed-toed shoes and slippers
(Mayo Clinic, 2022c)
(See also the Wild Iris Medical Education course “Diabetes Care: Prevention and Clinical Care of Diabetic Foot Ulcers.”)
EYE COMPLICATIONS
High blood glucose levels in patients with T1DM lead to an increased risk of eye complications. Although some of these complications may lead to blindness, many are only minor eye problems. The most serious diabetic diseases of the eye start with blood vessel problems. The four diseases that can threaten sight are:
- Diabetic retinopathy
- Diabetic macular edema
- Glaucoma
- Cataracts
(ADA, 2022a; Mayo Clinic, 2021c)
SYMPTOMS OF EYE COMPLICATIONS
- Blurry vision
- Difficulty reading signs or books
- Double vision
- Pain in one or both eyes
- Eye redness
- Feeling of pressure in the eye
- Seeing spots or “floaters”
- Straight lines appearing as not straight
- Disrupted peripheral vision
(Mayo Clinic, 2021c; Rebar et al., 2019)
The American Diabetes Association (2022a) recommends that persons with diabetes have regular eye examinations with an ophthalmologist or optometrist.
KIDNEY DISEASE (NEPHROPATHY)
Patients with T1DM have a high risk for the development of kidney disease. Because the kidney overworks to compensate for its decreased efficiency, early stages of kidney disease are often not accompanied by symptoms. Therefore, careful monitoring for signs of kidney deficiency at routine check-ups is an important component of care for patients with T1DM, and early intervention is a key step to limiting kidney damage (ADA, 2022a; Rebar et al., 2019).
SYMPTOMS OF NEPHROPATHY
- Loss of sleep
- Poor appetite
- Nausea and vomiting
- Weakness
- Difficulty concentrating
- Edema
- Pruritis
- Protein in the urine
- Fatigue
- Confusion
(Mayo Clinic, 2021c; Rebar et al., 2019)
The initial step in addressing diabetic nephropathy is to treat and control diabetes and hypertension. This includes adhering to the treatment plan, exercise, and dietary recommendations (Mayo Clinic, 2021e).
ADHESIVE CAPSULITIS (AC)
Commonly referred to as frozen shoulder, adhesive capsulitis is a condition marked by painful then increasingly restricted movement of the glenohumeral joint, with limitations most often occurring in the movements of external rotation and abduction. AC may be classified as primary (in cases that are idiopathic in nature) or secondary (in cases that result from a known cause) (Roberts, 2020).
SYMPTOMS OF ADHESIVE CAPSULITIS
Symptoms of AC usually have a slow onset with gradual worsening. Over time, symptoms usually resolve within 1–3 years. Symptoms include:
- Pain
- Limited range of motion
- Increasing stiffness
(Mayo Clinic, 2022d)
Research suggests that patients with diabetes are much more likely than the general population to have AC and are more resistant to treatment. Most cases of AC will spontaneously resolve over varying periods of time, but the resultant loss of motion during the affected period can significantly impact an individual’s ability to perform activities of daily living (ADLs) and other preferred functional activities.
Treatment for AC includes a range of options: corticosteroid injections, manipulation under anesthesia, translation mobilization under anesthesia, arthroscopic capsular release, and suprascapular nerve blocks. NSAIDs, oral steroids, and physical therapy evaluation/intervention are also frequently used in the treatment of AC (Roberts, 2020).
CONCLUSION
Type 1 diabetes mellitus is a serious disease whose chronic nature requires a lifelong commitment to therapy. Unlike T2DM, T1DM is caused by an autoimmune reaction, the results of which cause the body to be unable to properly store and process blood glucose. The hallmark clinical sign of T1DM is hyperglycemia; symptoms of hyperglycemia include increased thirst, blurred vision, frequent urination, and increased hunger.
While there are many strategies to manage T1DM, such as exercise and diet, the primary treatment is insulin therapy to make up for the lack of insulin production in these patients. Insulin administration allows patients to normalize their blood glucose levels. Tight control of blood glucose is an essential step to prevent the development and/or worsening of diabetes-related complications, a common occurrence in these patients.
The long-term therapy of patients with T1DM is best managed by a multidisciplinary care team composed of primary care providers, nurses, endocrinologists, and other specialists (i.e., cardiologists, ophthalmologists, dermatologists, podiatrists, physical therapists, occupational therapists, registered dietitians, and diabetes educators). Although there is currently no cure, with continued care and oversight as well as careful and committed adherence to lifestyle changes and treatments, patients with T1DM may experience an active and full life.
RESOURCES
Children with diabetes (Online community for kids, families, and adults with diabetes)
Device technology: better blood glucose meters and more (American Diabetes Association)
Diabetes type 1 (Medline Plus)
Exercise and type 1 (ADA)
Health fraud product database (U.S. FDA)
International Diabetes Federation
Planning meals (ADA)
What is the new technology for diabetes? (MedicineNet)
REFERENCES
NOTE: Complete URLs for references retrieved from online sources are provided in the PDF of this course.
Ambardekar N. (2021). High blood sugar and diabetes. WebMD. https://www.webmd.com
American Diabetes Association. (2022a). Standards of medical care in diabetes: 2022. Diabetes Care, 45(suppl 1). https://diabetesjournals.org
American Diabetes Association. (2022b). Statistics about diabetes. https://www.diabetes.org
American Diabetes Association. (2019). Diagnosis. https://www.diabetes.org
American Diabetes Association. (n.d.). Insulin pens. https://diabetes.org
Boshe et al. (2021). The magnitude of non-adherence and contributing factors among adult outpatient with diabetes mellitus in Dilla University Referral Hospital, Gedio Ethiopia. PLoS One, 16(3), e0247952. doi:10.1371/journal.pone.0247952
Buehler LA, Noe D, Knapp S, Isaacs D, & Pantalone KM. (2021). Ketogenic diets in the management of type 1 diabetes: Safe or safety concern? Cleveland Clinic Journal of Medicine, 88(10), 547–55. https://doi.org/10.3949/ccjm.88a.20121
Centers for Disease Control and Prevention (CDC). (2021a). The multidisciplinary DSMES team. https://www.cdc.gov
Centers for Disease Control and Prevention (CDC). (2021b). What is diabetes? https://www.cdc.gov
Centers for Disease Control and Prevention (CDC). (2021c). 4 ways to take insulin. https://www.cdc.gov
Cervoni B. (2022). What to expect from an islet cell transplant. Verywellhealth. https://www.verywellhealth.com
Cheng P, Dong Y, Hu Z, Huang S, Cao X, Wang P, Xu H, Zhu J, & Tang B. (2021). Biomarker prediction of postoperative healing of diabetic foot ulcers. Journal of Wound Ostomy and Continence Nursing, 48(4), 339–44. doi:10.1097/WON.0000000000000780
Cleveland Clinic. (2021). Diabetes-related ketoacidosis (DKA). https://my.clevelandclinic.org
Cleveland Clinic. (2020). Hyperglycemia (high blood sugar). https://my.clevelandclinic.org
Comerford M & Durkin T. (2022). Nursing 2022 drug handbook. Wolters Kluwer.
Dansinger M. (2020). Hemoglobin A1C (HbA1c) test for diabetes. WebMD. https://www.webmd.com
Diabetes.co.uk. (2022). Amylin analogues. https://www.diabetes.co.uk
Diabetes Research Institute. (2022). What is islet transplantation? https://www.diabetesresearch.org
Gilles G. (2022). What is estimated average glucose (eAG)? Verywellhealth. https://www.verywellhealth.com
JDRF. (2020). Type 1 diabetes facts. https://www.jdrf.org
Johns Hopkins Medicine. (2022). Pancreas transplantation. https://www.hopkinsmedicine.org
Khardori R. (2022). Type 1 diabetes mellitus. Medscape. https://emedicine.medscape.com
KidsHealth. (2022). Helping your child adjust to diabetes. https://kidshealth.org
Lakhanigam S. (2019). Continuous glucose monitoring systems reducing hypoglycemia and improving patient health outcomes. Minority Nurse. https://minoritynurse.com
Mayo Clinic. (2022a). Blood sugar testing: Why, when and how. https://www.mayoclinic.org
Mayo Clinic. (2022b). Pancreas transplant. https://www.mayoclinic.org/tests-procedures/pancreas-transplant/about/pac-20384783
Mayo Clinic. (2022c). Diabetic neuropathy. https://www.mayoclinic.org
Mayo Clinic. (2022d). Frozen shoulder. https://www.mayoclinic.org
Mayo Clinic. (2021a). Diabetes diet: Create your healthy-eating plan. https://www.mayoclinic.org
Mayo Clinic. (2021b). How much should the average adult exercise every day? https://www.mayoclinic.org
Mayo Clinic. (2021c). Type 1 diabetes. https://www.mayoclinic.org
Mayo Clinic. (2021d). Type 2 diabetes. https://www.mayoclinic.org
Mayo Clinic. (2021e). Diabetic nephropathy (kidney disease). https://www.mayoclinic.org
Mayo Clinic. (2020). Hyperglycemia in diabetes. https://www.mayoclinic.org
MedlinePlus. (n.d.). Type 1 diabetes. https://medlineplus.gov/
MedlinePlus. (2020). Portion size. https://medlineplus.gov
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). (2022). Insulin, medicines, & other diabetes treatments. https://www.niddk.nih.gov
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). (2021). Low blood glucose (hypoglycemia). https://www.niddk.nih.gov
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). (n.d.). The A1C test & diabetes. https://www.niddk.nih.gov
Pagana KD, Pagana TJ, & Pagana, TN. (2019). Mosby’s diagnostic and laboratory test reference (14th ed.). Elsevier.
Pinsker J. (2022). What is an insulin pump with an advanced hybrid closed-loop system? Tandem Diabetes Care. https://www.tandemdiabetes.com
Roberts JR. (2020). Adhesive capsulitis (frozen shoulder) treatment and management. Medscape. https://emedicine.medscape.com
Rebar CR, Heimgartner MM, & Gersch CJ (Eds). (2019). Pathophysiology made incredibly easy! (6th ed.). Wolters Kluwer.
Saini P. (2022). Importance of multidisciplinary care. Webmedy. https://webmedy.com
Torrey T. (2021). Why patients are non-compliant with treatment. Verywellhealth. https://www.verywellhealth.com
University of California, San Francisco (UCSF). (2022). Amylin analog treatment. https://dtc.ucsf.edu
UNC School of Medicine. (n.d.). Kidney and/or pancreas transplant overview: indications/contraindications. https://www.med.unc.edu
University Hospitals. (n.d.). When to refer a diabetic for pancreas transplant. https://www.uhhospitals.org
Vilarrasa N, San Jose P, Rubio MA, & Lecube A. (2021). Obesity in patients with type 1 diabetes: Links, risks, and management challenges. Diabetes Metab Syndr Obes, 14, 2807–27. doi:10.2147/DMSO.S223618
Waleed M. (2019). Patients are increasingly at risk for insulin-drug interactions. Pharmacy Times, 85(1). https://www.pharmacytimes.com
Customer Rating
5.0 / 459 ratings